
O2TRAINER SCIENCE
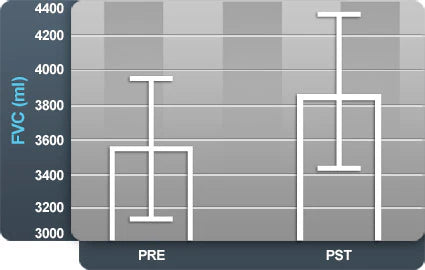
Forced Vital Capacity (FVC) Improvement
This graph shows average values for a measure of lung capacity referred to as forced vital capacity (FVC). As noted, FVC increased from pre to post after use of the O2Trainer.
Hematocrit (HCT) Increase
This graph shows the percent (%) of red blood cells in blood volume noted as hematocrit (HCT). As the graph indicates, pre to post values increase in HCT after use of the O2Trainer.
Clinical Research Results
Study: Nine (9) highly trained collegiate cross-country females participated. Five (5) were assigned as "experimental" indicating they would use the O2Trainer developed by Bas Rutten. The designated use of the device was 3 days per week during 5 kilometers of running.
NOTE: all the subjects stated that the device was NOT a hindrance to their training.
According to research done by the Rice University of Houston, altitude training has the following long term effects:
- Increased concentration of red blood cells
- Decreased maximum cardiac output with a decreased maximum heart rate, doing the same amount of work
- Red blood cells become more efficient at unloading oxygen to the tissues
ALL THE PARTICIPANTS IN THE TEST WHO USED AN O2TRAINER INCREASED THEIR VENTILATORY MUSCLES AND IMPROVED THEIR VOLUME OF AIR THEY COULD VENTILATE.
Study performed by:
Dr. Frank B. Wyatt, EPc
Professor/Graduate Coordinator
Department of Athletic Training & Exercise Physiology
Midwestern State University
College of Health Sciences and Human Services
Professor/Graduate Coordinator
Department of Athletic Training & Exercise Physiology
Midwestern State University
College of Health Sciences and Human Services
PLEASE READ PUBLISHED MEDICAL JOURNALS FOR AN IN-DEPTH LOOK AT THE O2TRAINER:






Sale price
$59.95
- Increased Endurance and Stamina
- Improved oxygen intake and efficiency
- Stronger respiratory muscles
- Enhanced performance for athletes and performers
- Made in the USA

